
Learn How AFib Increases Stroke Risk
Lower your risk of stroke
AFib is an abnormal heart rhythm. Your heart’s upper chambers (atria) beat in an abnormal pattern (fibrillate). You may feel unwell or experience a fluttering sensation in your chest. Or, you might not notice anything different at all.
During AFib, blood doesn’t move through your heart the way it normally does. Sometimes blood that doesn’t move through your heart can form a solid clump (clot). The clot can break off and travel through your bloodstream.
The clot can reach your brain and block blood flow. The blocked part of your brain can start to die. This is called a stroke. Strokes need immediate emergency medical treatment. You can die from a stroke, or it may leave you disabled.
Taking medication can help people with AFib lead full lives and reduce their risk of blood clots and stroke. Anticoagulants (blood thinners) are medications that can help prevent blood clots. Learn more about how blood thinners can reduce your stroke risk.

Make Informed Decisions for Better Health
Get answers in one click
Now, you can use a free online resource to better understand AFib and your options. It’s called the Stanford AFib Guide, and you can access it on your smartphone, tablet, or computer. You don’t need an app or special device. Here you’ll find:
- Short video that explains AFib and how blood thinners work
- Answers to common questions
- Quiz to test your AFib knowledge
- Stories from other patients with AFib
- A worksheet to encourage conversations between patients and their physicians
It’s easy to get started right away. Try the Stanford AFib Guide now
Work with your clinician to make a decision
Your clinician may recommend a blood thinner based on your risk of stroke. You and your clinician can work together to decide whether this type of medication is right for you. This decision can be reviewed with your clinician at any point.
It can be helpful to learn more about the benefits and risks of each choice before making a decision. Talking to your clinician and using the Stanford AFib Guide can help you make a choice that’s right for you.
Resources
AFib Stroke Prevention Website
Stanford AFib Guide Brochure
Blood Thinner Decision Worksheet
Patient Stories

From having a mini-stroke to being a more informed patient
Mrs. G is a 69-year-old white retired elementary school teacher. She was diagnosed with AFib after she had a mini-stroke. Mrs. G found the AFib resource very helpful. "It should be made available to all patients because it provided helpful images that improved my understanding". Before using the digital resource, Mrs. G’s AFib knowledge was 63%, but it improved to 100% after the visit. Mrs. G decided to take blood-thinners. Although she still had a few doubts about this decision, Mrs. G felt much more comfortable with her choice a month later.

Learning how to prevent a stroke after an AFib diagnosis
Mr. D is a 51-year-old African American FedEx driver. He and his wife of many years live with their two children. Mr. D has a history of type 2 diabetes and hypertension, and was diagnosed with AFib six months ago. He and his wife were enthusiastic about the Stanford AFib Guide: "This AFib website would have been beneficial earlier on." When Mr. D was introduced to the website, his doctor used it to discuss the risks of AFib, the benefits of blood thinners, and to illustrate what happens during a stroke. Mr. D’s AFib knowledge score rose from 63% before the appointment to 100% afterward. He also had the information he needed to make a clear decision about taking blood thinners.

Once skeptical about blood thinners, but now committed to taking them
Mrs. Y is a 73-year-old Chinese-American woman. Mrs. Y is widowed, and her three sons are very involved in her medical care. After she felt palpitations for the first time, Mrs. Y’s doctors detected AFib on a heart rate monitor. Mrs. Y was very impressed with the AFib website: "Most importantly, I believe the AFib resource will educate and benefit not only patients, but also the general public in a big way." Mrs. Y, her son, and her doctor discussed concerns about AFib, blood thinners, and stroke risk. She started out very skeptical about blood thinners, but left her appointment committed to taking them.
AFib and Blood Thinners: What to Consider
Whether to take blood thinners to reduce stroke risk is a very personal decision. There are many aspects to consider. We invite you to learn the facts about AFib and blood thinners.
Fact: For most people, the benefits of taking a blood thinner outweigh the downsides. Taking a blood thinner can prevent a stroke that might kill or disable you.
There are potential downsides to taking a blood thinner:
- Taking a blood thinner can make you bleed or bruise more easily.
- You’ll need to take precautions and avoid activities that increase your risk of falling or having a head injury.
- Cost and inconvenience can be downsides.
Depending on your own lifestyle and risk factors for stroke, these potential downsides may be more or less important for your decision.
Fact: Blood thinners are usually recommended for the rest of your life when you have AFib. But you can always discuss your concerns with your clinician if you wish to change your mind. You can work together to find other ways to reduce your stroke risk.
Fact: Most people are able to take blood thinners. Some people with high risk of bleeding, such as recent surgery, may need to wait before taking blood thinners.
It is important to ask your clinician if blood thinners are right for you. Stanford AFib Guide answers these and other questions about AFib, stroke risk, and blood thinners.
AFib and Blood Thinner Facts
- AFib can lead to a stroke, even if you don’t feel anything.
- Taking a blood thinner will greatly reduce your risk of stroke.
- For most people, the benefits of taking blood thinners outweigh the risks.
- Taking a blood thinner is your choice. You can always change your mind later.
Explore Cardiac Arrhythmia Care at Stanford Health Care
Stanford Medicine’s highly skilled clinicians have an international reputation for treating atrial fibrillation and other arrythmias. We offer comprehensive care and support to diagnose and provide care for patients with AFib.
You can access our expert care at Stanford Health Care Cardiac Arrhythmia Service and other locations. We are national leaders in research and the development of new treatment guidelines for heart conditions. Our goal is to bring these leading therapies to you.
To make an appointment with one of our arrhythmia specialists, call 650-723-7111.
For More Information
At least 2.7 million Americans are currently living with AFib, and that number could increase to 12.1 million by 2030. Despite effective treatments for AFib, treatment for many patients is not as successful as it could be.
Many patients don’t fully realize their increased risk of stroke due to AFib. When patients are underinformed, they may be less likely to follow their care plan as directed. These gaps in treatment can lead to strokes that are largely preventable.
Physicians at Stanford Health Care recognized this pervasive issue in AFib care and set out to address it with the Stanford AFib Guide. This innovative digital resource is designed to improve AFib care through patient education and empowerment, and to facilitate shared decision-making. A collaborative care process between patients and their providers.
Stanford AFib Guide was made possible with support from the Joe and Linda Chlapaty Stanford DECIDE Center and the American Heart Association Strategically Focused Research Network. The Stanford AFib Guide is backed by a randomized clinical trial, complete with patient interviews, and feedback on prototypes. The online website is free to physicians and their patients.
Our clinical trial began in 2019 and ended in August 2022. We rigorously tested the Stanford AFib Guide at Stanford University, East Carolina University, Ochsner Medical Center, Cleveland Clinic Foundation, and Cooper Health System/Rowan University. The clinical trial, ENHANCE-AF, included diverse patient populations and a variety of health care systems.
Principal investigators Paul J. Wang, MD, and Randall S. Stafford, MD, PhD, examined the factors AFib patients consider when deciding to take anticoagulation medication. Their study focused on identifying and eliminating barriers to shared decision-making. These can include low health literacy and patients’ dissatisfaction with their previous care, and providers’ lack of cultural understanding.
To help overcome these barriers in AFib care, Drs. Wang and Stafford spearheaded the creation of this shared decision-making website. The Stanford AFib Guide website allows AFib patients to:
- Learn about AFib and the risk of stroke
- Evaluate the pros and cons of blood-thinning medications
- Take an active, informed role in decisions about their care
The Stanford AFib Guide, presents information in English or Spanish using plain language that doesn’t downplay the complex aspects of stroke prevention. Its design accommodates patient diversity in health literacy and learning styles (auditory or visual). This shared decision-making resource presents a groundbreaking approach for empowering patients for years to come.
In the future, the collaborative decision-making model can be adapted to an infinite number of health care scenarios. Shared decision-making can:
- Reduce glaring disparities in health outcomes among patients of different races, ethnicities, and geographical locations
- Improve quality of care
- Fit seamlessly into the post-pandemic health care landscape
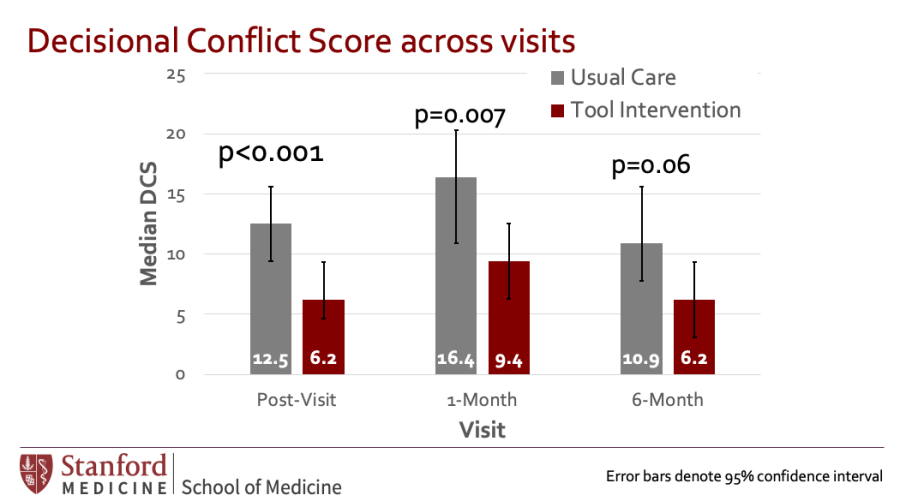
Drs. Wang and Stafford analyzed the trial’s results and shared findings on evaluating the impact of the website on patients’ views of the shared decision-making process at the American Heart Association’s Annual Scientific Sessions in November 2022. Results and publications from the Stanford AFib Guide clinical trial includes the following:
- The Stanford AFib Guide significantly decreased decisional conflict about the use of anticoagulation for atrial fibrillation stroke prevention (p=.007).
- Individuals using the Stanford AFib Guide showed significantly greater AFib knowledge (p<.001).
- Individuals were more prepared to make a decision about the use of anticoagulants (p<.001).
- Study results are available at www.ahajournals.org
- Find a complete list of publications here
Currently investigators are mining the clinical trial’s results for further insights, which include:
- Health care providers’ satisfaction with the shared decision-making process
- Patients’ general understanding of AFib
- Traditional clinical outcomes (such as stroke or gastrointestinal bleeding among study participants)
- The ways patients use the online resource over a longer period of time
The Stanford DECIDE Center will also collaborate on data analysis with the University of Utah DECIDE Center, which is currently conducting a shared decision-making research project with the Mayo Clinic.
Drs. Wang and Stafford are expanding the Stanford AFib Guide website capabilities to include all other aspects of AFib management, such as controlling heart rate and rhythm, and comprehensive strategies for preventing heart disease.
The Stanford DECIDE Center’s model of shared decision-making using a digital website is easily applicable to numerous health care topics:
- Under the American Heart Association’s Center for Health Technologies and Innovation, Dr. Wang is using insights from the Stanford DECIDE Center to develop digital resources for blood pressure management.
- Drs. Wang and Stafford will submit an NIH grant proposal to allow investigators to design and test a digital guide for older heart failure patients, focused on decision-making around having a cardioverter-defibrillator (ICD) implanted.
- The shared decision-making process is a natural fit for other chronic conditions, including but not limited to: heart failure, coronary artery disease, diabetes, hypertension, osteoarthritis. The Stanford AFib Guide website can help patients make informed decisions about medical treatment and procedures.
In each instance, the digital shared decision-making website can break down barriers to lead to more innovative, patient-centered care with better outcomes.
Clinician Resources
Who is ENHANCE-AF?
Paul J. Wang, MD, is director of the Joe and Linda Chlapaty DECIDE Center at Stanford University and a renowned expert in treating cardiac arrhythmias. Since 2003, he has served as director of the Stanford Cardiac Arrhythmia Service and as a professor of medicine and bioengineering at Stanford University. Dr. Wang’s research focuses on developing innovative approaches to treating arrhythmias, including less invasive therapies that improve and extend the lives of patients.
Randall S. Stafford, MD, PhD, is a professor of medicine at Stanford University School of Medicine and serves as director of the Program on Prevention Outcomes and Practices (PPOP). Dr. Stafford also serves as a primary care physician at Stanford Health Care where he focuses on the prevention and treatment of chronic diseases. His research is focused on creating effective health care models that emphasize prevention and wellness, rather than treatment of disease symptoms.








Publications
- Nunes JC, Baykaner T, Pundi K, DeSutter K, True Hills M, Mahaffey KW, Sears SF, Morin DP, Lin B, Wang PJ, Stafford RS. Design and development of a digital shared decision-making tool for stroke prevention in atrial fibrillation. JAMIA Open. 2023 Feb 2;6(1):ooad003. doi: 10.1093/jamiaopen/ooad003. PMID: 36751465; PMCID: PMC9893868.
- Nunes, J.C., Shah, S., Fazal, M. et al. Patient Education Strategies to Improve Risk of Stroke in Patients with Atrial Fibrillation. Curr Cardiovasc Risk Rep 16, 249–258 (2022). https://doi.org/10.1007/s12170-022-00709-8.
- Wang P, Lu Y, Mahaffey K, Lin A, Morin D, Sears S, Chung M, Russo A, et al. A Randomized Clinical Trial to Evaluate an Atrial Fibrillation Stroke Prevention Shared Decision-Making Pathway. J Am Heart Assoc. 2022; Nov 7: e8009. doi: 10.1161/JAHA.122.028562. Epub ahead of print. PMID: 36342828.
- Baykaner T, Pundi K, Lin B, Lu Y, DeSutter K, Morin D, et al. The ENHANCE-AF Clinical Trial to Evaluate an Atrial Fibrillation Shared Decision-Making Pathway: Rationale and Study Design. Am Heart J 2022 Jan 26:S0002-8703(22)00013-8. doi: 10.1016/j.ahj.2022.01.013. Online ahead of print. PMID: 35092723.
- Pourshams I, Lin B, Wang PJ, Stafford RS. Decision-Making Experiences and Decisional Regret in Patients Receiving Implanted Cardioverter-Defibrillators. Heart Mind 2022; 6(1): 32-5. doi: 10.4103/hm.hm_51_21 Abstract (no PMID yet)
- Chung MK, Wang PJ, Fagerlin A, Ajayi TB, Allen LA, Baykaner T, et al. Shared Decision Making in Cardiac Electrophysiology Procedures and Arrhythmia Management; Circ Arrhythm Electrophysiol, 2021 Dec;14(12):e007958. doi: 10.1161/CIRCEP.121.007958. Epub 2021 Dec 6. PMID: 34865518.
- Nunes JC, Rice EN, Stafford RS, Lewis EF, Wang PJ. Underrepresentation of Ethnic and Racial Minorities in Atrial Fibrillation Clinical Trials (Research Letter). Circ Arrhythm Electrophysiol, 2021; Nov 18: CIRCEP121010452. doi: 10.1161/CIRCEP.121.010452. Epub ahead of print. PMID: 34789014.
- Pundi K, Baykaner T, True Hills M, Lin B, Morin DP, Sears SF, et al. Blood Thinners for Atrial Fibrillation Stroke Prevention. Circ Arrhythm Electrophysiol. 2021 Jun;14(6):e009389. doi: 10.1161/CIRCEP.120.009389. Epub 2021 Jun 11. PMID: 34111936; PMCID: PMC8208521.
- Ajayi TB, Remein CD, Stafford RS, Fagerlin A, Chung MK, Childs E, et al. Cross-Center Virtual Education Fellowship Program for Early-Career Researchers in Atrial Fibrillation. Circ Arrhythm Electrophysiol. 2020 Nov;13(11):e008552. doi: 10.1161/CIRCEP.120.008552. Epub 2020 Oct 8. PMID: 33031707; PMCID: PMC7674267.
Bibliography
- Schnabel RB, Yin X, Gona P, et al. 50-year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet 2015;386(9989):154–62. doi:10.1016/S0140-6736(14)61774-8.
- Chugh SS, Blackshear JL, Shen WK, Hammill SC, Gersh BJ, et al. Epidemiology and natural history of atrial fibrillation: clinical implications. J. Am. Coll. Cardiol. 2001;37(2):371–8. doi:10.1016/s0735-1097(00)01107-4.
- Hsu JC, Freeman JV. Underuse of vitamin K antagonist and direct oral anticoagulants for stroke prevention in patients with atrial fibrillation: a contemporary review. Clin. Pharmacol. Ther. 2018;104:301–10.
- Chan PS, Maddox TM, Tang F, Spinler S, Spertus JA, et al.Practice-level variation in warfarin use among outpatients with atrial fibrillation (from the NCDR PINNACLE program). Am. J. Cardiol. 2011;108(8):1136–40. doi:10.1016/j.amjcard.2011.06.017.
- Seaburg L, Hess EP, Coylewright M, Ting HH, McLeod CJ,Montori VM, et al. Shared decision making in atrial fibrillation: where we are and where we should be going. Circulation 2014;129(6):704–10.
- Lip GYH, Nieuwlaat R, Pisters R, Lane DA, Crijns HJG, et al.Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach. Chest 2010;137:263–72.
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. J. Am. Coll. Cardiol. 2019;74(1):104–32.
- Holbrook A, Labiris R, Goldsmith CH, Ota K, Harb S, Sebaldt RJ, et al. Influence of decision aids on patient preferences for anticoagulant therapy: a randomized trial. CMAJ 2007;176(11):1583–7.
- McAlister FA, Man-Son-Hing M, Straus SE, et al. Impact of a patient decision aid on care among patients with nonvalvular atrial fibrillation: a cluster randomized trial. CMAJ 2005;173(5):496–501.
- Thomson RG, Eccles MP, Steen IN, et al. A patient decision aid to support shared decision-making on anti-thrombotic treatment of patients with atrial fibrillation: randomised controlled trial. Qual. Saf. Health Care 2007;16(3):216–23.
- Man-Son-Hing M, Laupacis A, O’Connor AM, et al. A patient decision aid regarding antithrombotic therapy for stroke prevention in atrial fibrillation: a randomized controlled trial. JAMA 1999;282(8):737–43.
- Institute of Medicine. Board on Population Health and Public Health Practice & Roundtable on Health Literacy. Health Literacy and Numeracy: Workshop Summary. National Academies Press; 2014.
- Aronis KN, Edgar B, Lin W, et al. Health literacy and atrial fibrillation: relevance and future directions for patient-centred care. Eur Cardiol Rev 2017;12:52.
- White S, Bennett I, Cordell T, Baxter SL. Health Literacy of America’s adults: results from the 2003 National assessment of adult literacy. PsycEXTRA Dataset 2007. doi:10.1037/e530912012-001.
- O’Connor AM. Validation of a decisional conflict scale. Med.Decis. Making 1995;15:25–30.
- Brehaut JC, O’Connor AM, Wood TJ, et al. Validation of a decision regret scale. Med. Decis. Making 2003;23(4):281–92.
- Pundi K, Baykaner T, True Hills M, et al. Blood thinners for atrial fibrillation stroke prevention. Circ. Arrhythm. Electrophysiol. 2021;14(6).
- Kunneman M, Branda ME, Noseworthy PA, et al. Shared decision making for stroke prevention in atrial fibrillation: study protocol for a randomized controlled trial. Trials 2017;18. doi:10.1186/s13063-017-2178-y.
- Shieh G, Jan S-L, Randles RH. On power and sample size determinations for the Wilcoxon–Mann–Whitney test. J.Nonparametr. Stat. 2006;18:33–43.
- Mollan KR, Trumble IM, Reifeis SA, et al. Precise and accurate power of the rank-sum test for a continuous outcome. J Biopharm Stat 2020;30:639–48.
- Kunneman M, Branda ME, Hargraves IG, et al. Assessment of shared decision-making for stroke prevention in patients with atrial fibrillation: a randomized clinical trial. JAMA Intern. Med.2020;180(9):1215–24.
- Berkman ND, Dewalt DA, Pignone MP, et al. Literacy and health outcomes, summary, evidence report. Technol Assess 2004;87.
- Magnani JW, Mujahid MS, Aronow HD, et al. Health literacy and cardiovascular disease: fundamental relevance to primary and secondary prevention: a scientific statement from the American Heart Association. Circulation 2018;138. doi:10.1161/cir.0000000000000579.
- Ryan JG, Leguen F, Weiss BD, et al. Will patients agree to have their literacy skills assessed in clinical practice? Health Educ. Res.2008;23(4):603–11.
- Baker DW, Wolf MS, Feinglass J, Thompson JA, Gazmararian JA, et al. Health literacy and mortality among elderly persons. Arch. Intern. Med. 2007;167(14):1503–9.
- Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice:update of a systematic review of health professionals’ perceptions. Patient Educ. Couns. 2008;73:526–35.