
Removing Tiny Filter Embedded in Vein Takes Expertise Unique to Stanford Hospital
01.12.2011
Over the years, Susan Karnstedt had gotten used to the intermittent pain in her abdomen, chalking it up to her diet, or perhaps to her physically active lifestyle, as a water skier and yoga enthusiast.
"The abdominal pain continued to get progressively worse, and was pretty debilitating," the 44-year-old Portola Valley resident said, describing how she was feeling when she visited the doctor earlier this year.
Karnstedt was well aware of her history of blood clots, but that still didn't prepare her for what she then learned: her pain could be traced to a filter that had been inserted more than 18 years ago in her inferior vena cava, the big vein that goes from the lower half of the body to the heart. Part of it was now poking through her intestines.
Removing this permanent-type umbrella-shaped device would not even be considered at most hospitals today, but Karnstedt was fortunate to be referred to interventional radiologist William Kuo, MD, at Stanford Hospital & Clinics. His team is believed to be the first in the world to apply endovascular laser technology to successfully retrieve permanently embedded IVC filters, and Stanford is currently the only hospital in the country where these procedures are routinely performed. "It is now possible to safely explant many of these devices that were previously irretrievable," Kuo said.
To fully appreciate Karnstedt's remarkable recovery, it's necessary to go back to 1992, when the device, known as a Greenfield Filter, was first inserted. She had gone to a Chicago emergency room barely able to breathe with pain and swelling in her left leg. There she was diagnosed with a life-threatening deep-venous thrombosis and pulmonary embolism — a blood clot that had formed in a vein in her pelvis and traveled to her lungs.
As part of the treatment, doctors inserted the Greenfield filter into her inferior vena cava, the big vein that carries deoxygenated blood from the lower half of the body to the heart.
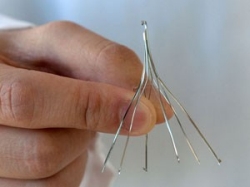
The metallic filter looks like an umbrella frame, with multiple spidery legs. Many doctors now recognize the difficulty with filters that are left in for a long time — they can eventually become the source of a new clot and shut down the inferior vena cava. What's more, the legs of the filter can erode through the IVC and puncture adjacent organs. It is believed that the risk of developing such complications increases the longer a filter remains in place.
But back in 1992, Karnstedt's IVC filter was thought to be harmless over a lifetime and was intended as a permanent implant.
Forward to 2010. Karnstedt and her family had moved to the Bay Area, where she consulted with a hematologist regarding a long-term anti-coagulation strategy in light of her high-risk condition. A CT scan was ordered to check that Karnstedt's IVC filter was free of clots, and that blood was flowing through stents that had been inserted into her iliac vein in the years following the 1992 procedure. What the scan turned up was unexpected and frightening.
Although no clots were identified, over the course of 18 years Karnstedt's IVC filter had turned lethal. "Over time, a few of the filter legs had eroded through, perforating her IVC, and one of them had impaled her intestines," said Kuo. "The filter tip had also become tilted and was embedded within the IVC wall. The degree of filter leg penetration through the intestines was shocking and undoubtedly the cause of her chronic and worsening abdominal pain." Karnstedt described it as a "fork poking" into her intestines.
Karnstedt also consulted with experts in her native Chicago where the filter was originally placed. According to Karnstedt, she was told that no one there had removed a non-retrievable filter and that permanent IVC filter removal had never been successfully accomplished. So she turned to Kuo and SHC.
As an interventional radiologist who specializes in vascular disease and management of complex IVC filter cases, Kuo has seen more and more patients referred to him from around the country for treatment of problematic IVC filters. These patients have inspired him to pioneer alternative methods that can be used to safely remove these devices. The cumulative results of years of research, coupled with ongoing studies, have resulted in new protocols for managing these challenging, high-risk cases in patients who otherwise would have no treatment option.
Kuo has published his data on complex and high-risk filter retrieval in the Journal of Vascular and Interventional Radiology, and he recently presented new data on use of his laser technique at this year's Society of Interventional Radiology meeting.
Kuo's expertise convinced him that he could potentially use these alternative methods to help Karnstedt who had by far the longest filter implant with the most severe intestinal perforation he had ever seen. "Every filter patient is unique, and thus the treatment must be meticulously planned and personalized to fit the patient," Kuo said.
On April 13, using real-time X-ray fluoroscopy to guide him, Kuo made a 4-mm incision in Karnstedt's neck, inserted a catheter into her jugular vein and guided it toward the filter in her vena cava. He then formed a special wire loop through the embedded filter and carefully began to realign it. The technique also allowed him to free the filter leg that had perforated through her intestines.
Next, through the same incision, Kuo advanced a special endovascular laser around the legs of the filter, and used this to carefully ablate the adherent tissues tethering the filter in place. This was a delicate maneuver as Kuo attempted to separate the scar tissue, which had formed around the filter over 18 years, without injuring the underlying normal vessel. After hours of working in this fashion, he was able to free, collapse, and completely remove the filter without damaging the underlying vena cava.
There was no need for open surgery, and following the procedure, no stitches were required—just a Band-aid on her neck site.
Side effects? "None," Karnstedt said. "I was done at 2 p.m., and home by 6 p.m., having dinner with my family."
For her part, the Portola Valley mom said she is happy to be pain free. "I could have gone to dance class the next morning," she said about the recovery time. Instead, she and her family celebrated with a stroll on the beach at Half Moon Bay.
About Stanford Health Care
Stanford Health Care, located in Palo Alto, California with multiple facilities throughout the region, is internationally renowned for leading edge and coordinated care in cancer, neurosciences, cardiovascular medicine, surgery, organ transplant, medicine specialties and primary care. Stanford Health Care is part of Stanford Medicine, which includes Lucile Packard Children's Hospital Stanford and the Stanford University School of Medicine. Throughout its history, Stanford has been at the forefront of discovery and innovation, as researchers and clinicians work together to improve health, alleviate suffering, and translate medical breakthroughs into better ways to deliver patient care. Stanford Health Care: Healing humanity through science and compassion, one patient at a time. For more information, visit: StanfordHospital.org.
CARE AT STANFORD
World-leading experts in diagnosis and advanced treatment deliver complete, compassionate, minimally invasive care for a wide range of cancers, vein and artery disorders, women’s health problems, and other conditions.
650-724-7362
Media Contacts
Lisa Kim
650-723-6696
likim@stanfordhealthcare.org