
Understanding A Woman's Heart Means Knowing What to Look For
01.12.2012
Reyna Robles was always the first one up and the last one to bed, the kind of person whose warmth and energy seemed effortless, possessed of more than enough steam to come home from her full-time job, to select recipes from her large collection of cookbooks to prepare a meal for her husband and children, and then to take her dogs for walk and help her kids with homework. Before bedtime, she'd fit in a good work out.
She wasn't one to complain, either, except the spring day when she suddenly felt a pain in her chest as she exercised. It was a cramp-like pain, not anything like the normal muscle aches Robles expected from her body after vigorous activity. "I didn't think I should be feeling chest pains," she said. She wasn't even 40.
She saw her doctor, who ordered an EKG. Everything was fine, Robles was told. Nothing was wrong with her heart. But the pain kept coming back, and that worried her. "Exercise should feel good," she said. "It shouldn't hurt." She went back to her doctor, who ordered more tests. Still nothing, she was told. Soon, she started feeling the pain even when she wasn't exercising. "I intuitively knew something wasn't right," she said. Still, none of the doctors she saw could discern a problem. And she began to doubt herself, "although I knew I wasn’t imagining it. It was real."
I intuitively knew something wasn't right. I knew I wasn't imagining it.
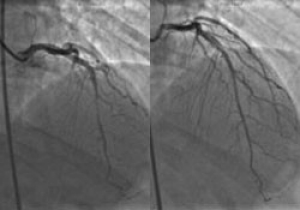
Robles' heart function was impaired by a physical anomaly called a myocardial bridge, where an artery is enveloped by heart muscle. When the heart muscle contracts, blood flow through that artery is constricted, too. On the left, a contracted heart; on the right, a relaxed heart.
With no answers and no end to the pain, Robles' whole view of life was gradually permeated by the uncertainty of her health. "I'm normally very positive, very bubbly and cheerful," she said, "but I felt like a shadow of my former self. All I could think about was my chest pain." By winter, she'd become desperate for help and went online to find it. She connected with a group of women who had experienced similar symptoms. One of them was a patient of Jennifer Tremmel, MD, Clinical Director of the Stanford Hospital Women's Heart Health program, just celebrating its fifth year in service.
Deceptively normal
In Tremmel, Robles found someone whose focused interest and knowledge of heart disease in women became the key to solving her medical mystery. "For years, the standard medical treatment for women with heart disease was based on what we know about heart disease in men," Tremmel said. "That's really confounded things. In the past 30 years, we've learned a lot about how women differ from men, but there's a lot we still don’t know. Just getting physicians to have a broader concept of symptoms, and what constitutes coronary artery disease in women, is a challenge."
Robles is a classic example of the challenge, in several ways. Her first EKG, stress test and angiogram were deemed normal. "What we have found is that stress tests, and even angiograms, may not always identify the problem in a woman's heart", Tremmel said. "If a lack of blood flow through the entire thickness of the heart muscle is needed to have a positive stress test, those patients with symptoms from a lack of blood flow to only the inner most lining of the heart may not be caught."
Similarly, Tremmel said, angiograms catch only blockages in large vessels, but patients, particularly women, may have a problem like endothelial dysfunction, which affects small vessels whose failure to work properly can't be seen on angiography.

After many frustrating visits to doctors who told her they could find nothing wrong, Robles found Jennifer Tremmel, MD, who leads the Women's Heart Health at Stanford Program.
Robles came to Stanford as many do, having been told no abnormalities had been found. Yet her symptoms were still there. "We decided we'd look harder," Tremmel said. "We did all this extra testing to see if we might find something that had been missed on her original angiogram."
Tremmel discovered that Robles had a physical anomaly called a myocardial bridge, where an artery that normally sits on top of the heart actually dives down into the heart muscle. Such bridges are not uncommon, and most people can live their entire lives without symptoms, but if a large portion of the artery is deeply buried, then there's trouble. Again, however, this physical abnormality often doesn't show up on an angiogram.
What we have found is that stress tests, and even angiograms, may not always identify the problem.
|
1
HEART ATTACK SYMPTOMS WOMEN SHOULD KNOW |
|---|
|
1
Chest pain is the classic signal of heart failure, but that can also feel like pressure, tightness, squeezing or burning. Other symptoms might also be part of an attack in a woman.
Preventing a heart attack
Diagnostic Tests to Consider
|
Trouble uncovered
Finally, with no other options left, Tremmel began to consider a surgery to release the artery from the muscle. "The surgery itself isn't complicated," she said, "but it is open heart surgery where you open the chest and expose the heart. It's a big deal. But for patients who have a poor quality of life, and you can't find any other way, it's a viable option."
Before the final decision was made, Tremmel wanted to do one more test. She inserted a wire into Robles' artery, while stressing her heart with medication, to measure the pressure and flow, on that one particular part of her heart's anatomy. "The test proved that the bridge was definitely the problem," Tremmel said. Tremmel’s colleague, cardiovascular surgeon Michael Fishbein, MD, made the repair to Robles' heart.
Less than a month after her surgery, Robles was taking small but steady steps toward a more active life. After so many months of living with fear and uncertainty, Robles' belief in the strength of her repaired heart has been helped along by Tremmel's gentle encouragements. Robles worried aloud at a recent exam about some enthusiastic laughing she'd done with one of her daughters, so exuberant that her chest began to hurt. Tremmel pressed her stethoscope against Robles' chest for a close listen.
We pride ourselves in taking the time to really figure out what's going on, and not just saying there are no blockages.

As she recovers from surgery to reroute an artery covered by heart muscle, Robles has returned with gusto to cooking, much to the appreciation of her husband, Martin.
"It sounds like a happy heart," said Tremmel. "You can laugh as much as you want."
Re-entry
"I'm so very grateful to her," Robles said, "and to my whole care team at Stanford. I will never stop being grateful. I am blessed every day. It can be difficult to find a doctor willing to listen. Dr. Tremmel never ever gave up."
"We pride ourselves in taking the time to really figure out what's going on," Tremmel said, "and not just saying there are no blockages, that everything must be fine. The technique we use in the cath lab, for instance, is available to any physician out there, but it's really a matter of learning how to do these things and taking the time. It is more time consuming than a simple angiogram."
Beyond accurate diagnosis, she said, "you also have to stick with your patients. There's no magic bullet to make them feel better. It's a multi-factorial approach of using medications that improve symptoms, as well as encouraging lifestyle changes and stress reduction."
"The Stanford Women's Heart Health program staff includes a psychologist," Tremmel said. "There's a great deal of emotional stress that comes along with having these symptoms that nobody could explain for a long time. That in itself is a huge burden. A lot of women come to us with years of having people tell them, 'There's nothing there.' They doubt themselves and have really been affected by that. I think addressing all these factors is important."
CARE AT STANFORD
We provide exceptional heart care that starts with the understanding that women’s bodies have different needs—treating the whole woman using evidenced-based approaches to prevent and treat heart disease.
650-725-5909