
Thymoma Surgery
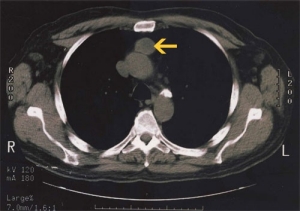
CT scan image of a well-circumscribed, anterior mediastinal thyoma.
Thymomas are malignant tumors that arise in the thymus gland, typically in the anterior mediastinum. Although considered malignant, most thymomas grow slowly and tend to spread only locally, by "seeding" cells into surrounding tissues and spaces such as the pleural space (the space surrounding each lung). There is therefore often a very good chance of curing thymomas by either surgery alone or surgery followed by radiation. We often proceed to remove these localized tumors without even the need for a preliminary biopsy.
More difficult thymic tumors that consist of frank carcinoma cells, and other thymic tumors that appear to invade surrounding structures on preoperative radiographic studies, are often best treated by administering preoperative chemotherapy or chemotherapy and radiation before surgical removal. These cases are discussed at our multidisciplinary Thoracic Tumor Board which consists of specialists from oncology, radiation oncology, radiology, and pathology in addition to thoracic surgeons. Here, the optimal treatment plan can be designed with the combined input from all the appropriate experts. These tumors require a preoperative needle biopsy or surgical biopsy to confirm the diagnosis before giving preoperative therapies. Surgery is then generally carried out if it is felt to be possible and there has been at least some shrinkage in response to the preoperative treatment.
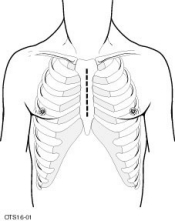
The skin incision for a median sternotomy—the typical incision for removal of a thymoma.
The most common surgical incision through which to remove a thymoma is a median sternotomy. This is a vertical incision through the breast bone that provides excellent exposure of the anterior mediastinum. Since no chest wall muscles are cut with this incision, postoperative pain is modest, and recovery is not prolonged. Smaller thymomas may be treated with VATS (video-assisted thoracoscopic surgery)(thymectomy), but this is an emerging area that we are moving into cautiously, with patient-safety at the forefront of our minds. We are also among the most experienced centers in transcervicalthymectomy for myasthenia gravis, but we believe this approach should be reserved primarily for patients without thymoma—it should certainly not be used for more than the smallest thymomas (less than 2 cm in size) given the risk of spillage of tumor cells.