
Types
Our Approach
Cardiac catheterization offers precise evaluation of your heart’s blood vessels and pressures, determining when you need treatment and when you do not. We use cardiac catheterization to accurately diagnose the cause of heart-related symptoms, including chest pain, dizziness, fatigue, shortness of breath, or any combination of these symptoms.
We perform 4,000 catheterizations each year. Stanford's heart doctors develop or help refine many heart tests and procedures, with several not widely available. Our sophisticated cardiac catheterization lab uses low-radiation, high-resolution digital equipment to maximize your safety and image quality. Our radial technique (through the wrist) improves comfort and reduces recovery time.
What Is Cardiac Catheterization?
To request an appointment with an interventional cardiologist, call 650-725-2621.
Types of Cardiac Catheterization
In addition to treatments such as angioplasty and stenting and heart valve repair or replacement, we perform a full range of diagnostic tests using cardiac catheterization. These minimally invasive tests, some of which are not widely available, include:
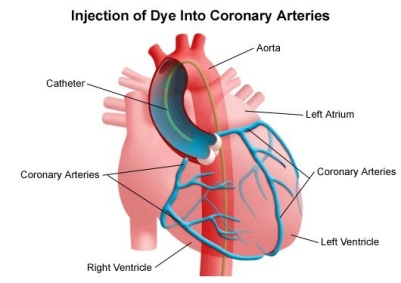
- Coronary angiogram or angiography: The most common catheterization test looks for the blocked arteries typically associated with heart disease. A cardiologist injects a special contrast dye that shows up on low-dose X-rays and tracks the flow of blood. The cardiologist can pinpoint blocked or narrowed arteries, assess the severity of the condition, and determine what type of treatment, if any, is needed.
- Fractional flow reserve (FFR): This test can help clarify the need for treatment, if a standard angiogram shows that an artery is only modestly narrowed. We thread a wire with a pressure sensor past the spot in question, to compare blood flow and pressure on each side. We can determine when you need a stent and when medication alone is enough. Our doctors continue to study this technique and participate in clinical trials, leading many of them. They have pioneered techniques to perform the tests, as well as the methods for interpreting and applying the results.
- Intravascular ultrasound (IVUS): We attach an ultrasound probe to the end of a catheter to see inside arteries and make measurements if the vessels are narrowed or blocked. This technique often provides more information than a standard angiogram and can help plan the most appropriate treatment. We can also evaluate suspected bridging, when an artery sits under heart muscle rather than on top. Stanford researchers pioneered IVUS, and it remains a highly precise tool for detecting and evaluating coronary artery disease.
- Optical coherence tomography (OCT): Like intravascular ultrasound, OCT uses a probe, but one that emits light waves instead of sound waves. OCT offers much greater resolution than IVUS, with the ability to see tiny details inside an artery. Our doctors continue to study the best way this technology can improve patient care.
- Vascular function testing: If you feel chest pain but your coronary arteries look clear on a standard angiogram, we may perform further, highly specialized testing:
- Endothelial function testing: This test examines the endothelial cells that line your coronary arteries, controlling when they contract and relax. A cardiologist injects a drug to see how the vessels react and to analyze whether they work properly. Those that do not may play a role in heart attack, as well as the thickening and hardening of arteries called atherosclerosis. We are among the few programs in the country offering this testing.
- Index of microcirculatory resistance: The index is the most accurate method for measuring the health of the tiny branches (microvasculature) of the coronary arteries, a challenging evaluation. The branches play a crucial role in delivering oxygen-rich blood but are too small to appear on an angiogram. Created by one of our doctors, the index is calculated by gauging blood pressure and flow after injecting a special drug. We use the latest, specialized wires to take those measurements.
What to Expect
Before
During
After
Before the Procedure
The doctor will explain the procedure and offer the opportunity to ask questions about the procedure.
Patients will be asked to sign a consent form that gives permission to do the test. It's important to read the form carefully and to ask questions if something is not clear.
Fasting is necessary prior to the procedure. Patients will be notified about how long to fast, usually overnight.
Patients should notify their doctor of the following:
- Previous reaction to any contrast dye, or allergies to iodine or seafood
- Sensitivities or allergies related to any medications, latex, tape, and anesthetic agents (local and general)
- Pregnancy or suspected pregnancy
- Body piercings on the chest and/or abdomen
- All current medications (prescription and over-the-counter) and herbal supplements
- If the patient has heart valve disease, the patient may need to receive an antibiotic prior to the procedure
- History of bleeding disorders or if the patient is taking any anticoagulant (blood-thinning) medications, aspirin, or other medications that affect blood clotting. It may be necessary for the patient to stop some of these medications prior to the procedure.
- If the patient has a pacemaker
The doctor may request a blood test prior to the procedure to determine how long it takes blood to clot. Other blood tests may be done as well.
Patients may receive a sedative prior to the procedure to help with relaxation. If a sedative is given, patients will need someone to drive them home after the test.
The area around the catheter insertion site (groin area) may be shaved.
Based upon certain medical conditions, the doctor may request other specific preparation.
During the Procedure
A cardiac catheterization may be performed on an outpatient basis or as part of a hospital stay. Procedures may vary depending on patients' condition and their doctors' practices.
Generally, a cardiac catheterization follows this process:
- Patients will be asked to remove any jewelry or other objects that may interfere with the procedure. Patients may wear dentures or hearing aids.
- Patients will be asked to remove clothing and will be given a gown to wear.
- Patients will be asked to empty their bladder prior to the procedure.
- An intravenous (IV) line will be started in the patients hand or arm prior to the procedure for injection of medication and to administer IV fluids, if needed.
- Patients will be placed in a supine (on your back) position on the procedure table
- Patients will be connected to an ECG monitor that records the electrical activity of the heart and monitors the heart during the procedure using small, adhesive electrodes. Vital signs (heart rate, blood pressure, breathing rate, and oxygenation level) will be monitored during the procedure
- There will be several monitor screens in the room, showing vital signs, the images of the catheter being moved through the body into the heart, and the structures of the heart as the dye is injected.
- Patients will receive a sedative medication in their IV before the procedure to help with relaxation. However, patients will likely remain awake during the procedure.
- Pulses below the catheter insertion site will be checked and marked so that the circulation to the limb below the site can be checked after the procedure.
- A local anesthetic will be injected into the skin at the insertion site. Patients may feel some stinging at the site for a few seconds after the local anesthetic is injected.
- Once the local anesthetic has taken effect, a sheath, or introducer, will be inserted into the blood vessel. This is a plastic tube through which the catheter will be inserted into the blood vessel and advanced into the heart. If the arm is used, a small incision (cut) may be made to expose the blood vessel for insertion of the sheath.
- The catheter will be advanced through the aorta to the left side of the heart. Fluoroscopy will be used to assist in advancing the catheter to the heart.
- Once the catheter is in place, contrast dye will be injected through the catheter to visualize the heart and the coronary arteries. Patients may feel some effects when the contrast dye is injected into the IV line. These effects may include a flushing sensation, a salty or metallic taste in the mouth, and/or a brief headache. These effects usually last for a few moments.
- Patients should notify their doctor of any breathing difficulties, sweating, numbness, nausea and/or vomiting, chills, itching, or heart palpitations.
- After the contrast dye is injected, a series of rapid, sequential X-ray images of the heart and coronary arteries will be made. You may be instructed to take in a deep breath and hold it for a few seconds during this time.
- Once sufficient information has been obtained, the catheter will be removed. The insertion site may be closed with a closure device that uses collagen to seal the opening in the artery, use of sutures, or by applying manual pressure over the area to keep the blood vessel from bleeding. The doctor will determine which method is appropriate for the patient
- If a closure device is used, a sterile dressing will be applied to the site. If manual pressure is used, the doctor (or an assistant) will hold pressure on the insertion site so that a clot will form. Once the bleeding has stopped, a very tight bandage will be placed on the site. A small sandbag or other type of weight may be placed on top of the bandage for additional pressure on the site, especially if the site is in the groin.
- Patients will be assisted to slide from the table onto a stretcher so they can be taken to the recovery area. If the insertion was in the groin, patients will not be allowed to bend their leg for several hours.
To help patients remember to keep their leg straight, the knee of the affected leg may be covered with a sheet and the ends tucked under the mattress on both sides of the bed to form a type of loose restraint. If the insertion site was in the arm, it will be kept elevated on pillows and kept straight by placing the arm in an arm guard (a plastic arm board designed to immobilize the elbow joint).
In addition, a plastic band (works like a belt around the waist) may be secured around the patient's arm near the insertion site. The band will be loosened at given intervals and removed at the appropriate time as determined by the doctor.
After the Procedure
In the Hospital
After the procedure, patients may be taken to the recovery room for observation or returned to their hospital room.
They will remain flat in bed for several hours after the procedure. A nurse will monitor vital signs, the insertion site, and circulation/sensation in the affected leg or arm.
Patients should immediately inform the nurse of any chest pain or tightness, or any other pain, as well as any feelings of warmth, bleeding, or pain at the insertion site.
Bedrest may vary from two to six hours depending on the patient's condition. If the doctor placed a closure device, bedrest may be of shorter duration.
In some cases, the sheath or introducer may be left in the insertion site. If so, the period of bedrest will be prolonged until the sheath is removed. After the sheath is removed, patients may be given a light meal. Patients may feel the urge to urinate frequently because of the effects of the contrast dye and increased fluids. Patients will need to use a bedpan or urinal while on bedrest so that the affected leg or arm will not be bent.
After the specified period of bed rest has been completed, patients may get out of bed. The nurse will assist patients the first time they get up, and will check blood pressure while lying in bed, sitting, and standing. Patients should move slowly when getting up from the bed to avoid any dizziness from the long period of bedrest.
Patients may be given pain medication for pain or discomfort related to the insertion site or having to lie flat and still for a prolonged period.
Patients will be encouraged to drink water and other fluids to help flush the contrast dye from the body.
Patients may resume their usual diet after the procedure, unless the doctor decides otherwise.
When patients have completed the recovery period, they may be discharged unless their doctor decides otherwise. If this procedure was performed on an outpatient basis, patients must have another person drive them home.
At Home
Once at home, patients should monitor the insertion site for bleeding, unusual pain, swelling, and abnormal discoloration or temperature change at or near the insertion site. A small bruise is normal. If patients notice a constant or large amount of blood at the site that cannot be contained with a small dressing, notify the doctor.
If the doctor used a closure device at insertion site, patients will be given specific information regarding the type of closure device that was used and how to take care of the insertion site. There will be a small knot, or lump, under the skin at the site. This is normal. The knot should gradually disappear over a few weeks.
It will be important to keep the insertion site clean and dry. The doctor will give specific bathing instructions. Patients may be advised not to participate in any strenuous activities. The doctor will provide instructions about returning to work and resuming normal activities.
Notify the doctor to report any of the following:
- Fever and/or chills
- Increased pain, redness, swelling, or bleeding or other drainage from the insertion site
- Coolness, numbness and/or tingling, or other changes in the affected extremity
- Chest pain/pressure, nausea and/or vomiting, profuse sweating, dizziness, and/or fainting
The doctor may give additional or alternate instructions after the procedure, depending on the patients' needs.
Before the Procedure
The doctor will explain the procedure and offer the opportunity to ask questions about the procedure.
Patients will be asked to sign a consent form that gives permission to do the test. It's important to read the form carefully and to ask questions if something is not clear.
Fasting is necessary prior to the procedure. Patients will be notified about how long to fast, usually overnight.
Patients should notify their doctor of the following:
- Previous reaction to any contrast dye, or allergies to iodine or seafood
- Sensitivities or allergies related to any medications, latex, tape, and anesthetic agents (local and general)
- Pregnancy or suspected pregnancy
- Body piercings on the chest and/or abdomen
- All current medications (prescription and over-the-counter) and herbal supplements
- If the patient has heart valve disease, the patient may need to receive an antibiotic prior to the procedure
- History of bleeding disorders or if the patient is taking any anticoagulant (blood-thinning) medications, aspirin, or other medications that affect blood clotting. It may be necessary for the patient to stop some of these medications prior to the procedure.
- If the patient has a pacemaker
The doctor may request a blood test prior to the procedure to determine how long it takes blood to clot. Other blood tests may be done as well.
Patients may receive a sedative prior to the procedure to help with relaxation. If a sedative is given, patients will need someone to drive them home after the test.
The area around the catheter insertion site (groin area) may be shaved.
Based upon certain medical conditions, the doctor may request other specific preparation.
close Before
During the Procedure
A cardiac catheterization may be performed on an outpatient basis or as part of a hospital stay. Procedures may vary depending on patients' condition and their doctors' practices.
Generally, a cardiac catheterization follows this process:
- Patients will be asked to remove any jewelry or other objects that may interfere with the procedure. Patients may wear dentures or hearing aids.
- Patients will be asked to remove clothing and will be given a gown to wear.
- Patients will be asked to empty their bladder prior to the procedure.
- An intravenous (IV) line will be started in the patients hand or arm prior to the procedure for injection of medication and to administer IV fluids, if needed.
- Patients will be placed in a supine (on your back) position on the procedure table
- Patients will be connected to an ECG monitor that records the electrical activity of the heart and monitors the heart during the procedure using small, adhesive electrodes. Vital signs (heart rate, blood pressure, breathing rate, and oxygenation level) will be monitored during the procedure
- There will be several monitor screens in the room, showing vital signs, the images of the catheter being moved through the body into the heart, and the structures of the heart as the dye is injected.
- Patients will receive a sedative medication in their IV before the procedure to help with relaxation. However, patients will likely remain awake during the procedure.
- Pulses below the catheter insertion site will be checked and marked so that the circulation to the limb below the site can be checked after the procedure.
- A local anesthetic will be injected into the skin at the insertion site. Patients may feel some stinging at the site for a few seconds after the local anesthetic is injected.
- Once the local anesthetic has taken effect, a sheath, or introducer, will be inserted into the blood vessel. This is a plastic tube through which the catheter will be inserted into the blood vessel and advanced into the heart. If the arm is used, a small incision (cut) may be made to expose the blood vessel for insertion of the sheath.
- The catheter will be advanced through the aorta to the left side of the heart. Fluoroscopy will be used to assist in advancing the catheter to the heart.
- Once the catheter is in place, contrast dye will be injected through the catheter to visualize the heart and the coronary arteries. Patients may feel some effects when the contrast dye is injected into the IV line. These effects may include a flushing sensation, a salty or metallic taste in the mouth, and/or a brief headache. These effects usually last for a few moments.
- Patients should notify their doctor of any breathing difficulties, sweating, numbness, nausea and/or vomiting, chills, itching, or heart palpitations.
- After the contrast dye is injected, a series of rapid, sequential X-ray images of the heart and coronary arteries will be made. You may be instructed to take in a deep breath and hold it for a few seconds during this time.
- Once sufficient information has been obtained, the catheter will be removed. The insertion site may be closed with a closure device that uses collagen to seal the opening in the artery, use of sutures, or by applying manual pressure over the area to keep the blood vessel from bleeding. The doctor will determine which method is appropriate for the patient
- If a closure device is used, a sterile dressing will be applied to the site. If manual pressure is used, the doctor (or an assistant) will hold pressure on the insertion site so that a clot will form. Once the bleeding has stopped, a very tight bandage will be placed on the site. A small sandbag or other type of weight may be placed on top of the bandage for additional pressure on the site, especially if the site is in the groin.
- Patients will be assisted to slide from the table onto a stretcher so they can be taken to the recovery area. If the insertion was in the groin, patients will not be allowed to bend their leg for several hours.
To help patients remember to keep their leg straight, the knee of the affected leg may be covered with a sheet and the ends tucked under the mattress on both sides of the bed to form a type of loose restraint. If the insertion site was in the arm, it will be kept elevated on pillows and kept straight by placing the arm in an arm guard (a plastic arm board designed to immobilize the elbow joint).
In addition, a plastic band (works like a belt around the waist) may be secured around the patient's arm near the insertion site. The band will be loosened at given intervals and removed at the appropriate time as determined by the doctor.
close During
After the Procedure
In the Hospital
After the procedure, patients may be taken to the recovery room for observation or returned to their hospital room.
They will remain flat in bed for several hours after the procedure. A nurse will monitor vital signs, the insertion site, and circulation/sensation in the affected leg or arm.
Patients should immediately inform the nurse of any chest pain or tightness, or any other pain, as well as any feelings of warmth, bleeding, or pain at the insertion site.
Bedrest may vary from two to six hours depending on the patient's condition. If the doctor placed a closure device, bedrest may be of shorter duration.
In some cases, the sheath or introducer may be left in the insertion site. If so, the period of bedrest will be prolonged until the sheath is removed. After the sheath is removed, patients may be given a light meal. Patients may feel the urge to urinate frequently because of the effects of the contrast dye and increased fluids. Patients will need to use a bedpan or urinal while on bedrest so that the affected leg or arm will not be bent.
After the specified period of bed rest has been completed, patients may get out of bed. The nurse will assist patients the first time they get up, and will check blood pressure while lying in bed, sitting, and standing. Patients should move slowly when getting up from the bed to avoid any dizziness from the long period of bedrest.
Patients may be given pain medication for pain or discomfort related to the insertion site or having to lie flat and still for a prolonged period.
Patients will be encouraged to drink water and other fluids to help flush the contrast dye from the body.
Patients may resume their usual diet after the procedure, unless the doctor decides otherwise.
When patients have completed the recovery period, they may be discharged unless their doctor decides otherwise. If this procedure was performed on an outpatient basis, patients must have another person drive them home.
At Home
Once at home, patients should monitor the insertion site for bleeding, unusual pain, swelling, and abnormal discoloration or temperature change at or near the insertion site. A small bruise is normal. If patients notice a constant or large amount of blood at the site that cannot be contained with a small dressing, notify the doctor.
If the doctor used a closure device at insertion site, patients will be given specific information regarding the type of closure device that was used and how to take care of the insertion site. There will be a small knot, or lump, under the skin at the site. This is normal. The knot should gradually disappear over a few weeks.
It will be important to keep the insertion site clean and dry. The doctor will give specific bathing instructions. Patients may be advised not to participate in any strenuous activities. The doctor will provide instructions about returning to work and resuming normal activities.
Notify the doctor to report any of the following:
- Fever and/or chills
- Increased pain, redness, swelling, or bleeding or other drainage from the insertion site
- Coolness, numbness and/or tingling, or other changes in the affected extremity
- Chest pain/pressure, nausea and/or vomiting, profuse sweating, dizziness, and/or fainting
The doctor may give additional or alternate instructions after the procedure, depending on the patients' needs.
close After
Our Clinics
 300 Pasteur Drive 3rd Floor, Clinic A31
300 Pasteur Drive
300 Pasteur Drive 3rd Floor, Clinic A31
300 Pasteur Drive3rd Floor, Clinic A31
Stanford, CA 94305
Phone: 650-725-2621 Getting Here