
Putting a Number on It: The Risk from an Exposure to HIV
This information was provided by CATIE (the Canadian AIDS Treatment Information Exchange). For more information, contact CATIE at 1-800-263-1638.
Author: James Wilton
Service providers working in HIV prevention are often asked by their patients and clients about the risk of HIV transmission from an exposure to HIV through sex. What do the latest studies tell us about this risk? And how should we interpret and communicate the results?
Challenges in calculating a number
It isn't easy for researchers to calculate the risk of transmission from an exposure to HIV through sex. To do this effectively, a group of HIV-negative individuals need to be followed over time and their exposures to HIV—both the number of times they are exposed and the types of exposure—need to be tracked.
As you can imagine, accurately tracking the number of times a person is exposed to HIV is very difficult. Researchers ask HIV-negative individuals enrolled in these studies to report how many times they have had sex in a given period of time, what type of sex they had, how often they used condoms and the HIV status of their partner(s). Because a person may have trouble remembering their sexual behaviour or may not want to tell the whole truth, this reporting is often inaccurate.
Furthermore, a person does not always know the HIV status of their partner(s). For this reason, researchers usually enroll HIV-negative individuals who are in stable relationships with an HIV-positive partner (also known as serodiscordant couples). Researchers can then conclude that any unprotected sex reported by a study participant counts as an exposure to HIV.
Several studies have aimed to estimate the average risk of HIV transmission from a specific type of unprotected sex (for example, vaginal/anal/oral; insertive/receptive). Due to the difficulties of calculating this risk, these studies have produced a wide range of numbers. To come up with a more accurate estimate for each type of unprotected sex, some researchers have combined the results of individual studies into what is known as a meta-analysis.
All exposures are not equal
The results of several meta-analyses suggest that some types of sex carry on average a higher risk of HIV transmission than others. Below are estimates from meta-analyses that have combined the results of studies conducted in high-income countries. For types of sex where meta-analysis estimates do not exist, numbers from individual studies are provided.
Anal sex
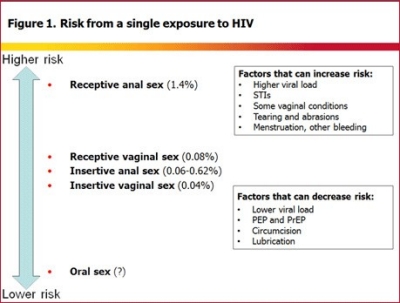
A meta-analysis exploring the risk of HIV transmission through unprotected anal sex was published in 2010.1 The analysis, based on the results of four studies, estimated the risk through receptive anal sex (receiving the penis into the anus, also known as bottoming) to be 1.4%. (This means that an average of one transmission occurred for every 71 exposures.) This risk was similar regardless of whether the receptive partner was a man or woman.
No meta-analysis estimates currently exist for insertive anal sex (inserting the penis into the anus, also known as topping) but two individual studies were conducted to calculate this risk. The first, published in 1999, calculated the risk to be 0.06% (equivalent to one transmission per 1,667 exposures).2 However, due to the design of the study, this number likely underestimated the risk of HIV transmission. The second study, published in 2010, was better designed and estimated the risk to be 0.11% (or 1 transmission per 909 exposures) for circumcised men and 0.62% (1 transmission per 161 exposures) for uncircumcised men.3
Vaginal sex
A meta-analysis of 10 studies exploring the risk of transmission through vaginal sex was published in 2009.4 It is estimated the risk of HIV transmission through receptive vaginal sex (receiving the penis in the vagina) to be 0.08% (equivalent to 1 transmission per 1,250 exposures).
A meta-analysis of three studies exploring the risk from insertive vaginal sex (inserting the penis into the vagina) was estimated to be 0.04% (equivalent to 1 transmission per 2,500 exposures).4
Oral sex
No meta-analysis estimates exist for oral sex (vaginal or penile) because too few good-quality studies have been completed. This is because it is difficult to find people whose only risk of HIV transmission is unprotected oral sex. A review of the studies that are available was published in 2008 and concluded that vaginal and penile oral sex pose a "low but non-zero transmission probability."5
In the three studies aimed at calculating the risk of HIV transmission from one act of oral sex, no transmissions were observed among three different populations—lesbian serodiscordant couples, heterosexual serodiscordant couples and single gay men—who reported unprotected oral sex as their only risk for HIV transmission. However, these studies enrolled only a small number of people and followed them for only a short period of time, which may explain the lack of HIV transmissions and makes it impossible to conclude that the risk from oral sex is zero.
Risk of HIV transmission from different types of unprotected sex
|
1
|
1
Number of individual studies |
1
Range of estimates |
1
Meta-analysis estimate |
|---|---|---|---|
|
1
Receptive anal |
1
4 |
1
0.4% - 3.38% |
1
1.4% |
|
1
Insertive anal |
1
2 |
1
0.06% - 0.62% |
1
- |
|
1
Receptive vaginal |
1
10 |
1
0.018% - 0.150% |
1
0.08% |
|
1
Insertive vaginal |
1
3 |
1
0.03% - 0.09% |
1
0.04% |
Interpreting the numbers—what additional information needs to be provided?
Some clients may see these numbers and think their risk of HIV transmission is low. Therefore, caution is needed when interpreting them. If these numbers are provided to clients, they should be accompanied by information that helps shed light on why the risk may be higher than it seems.
Transmission can occur after one exposure.
It is important to emphasize that a person could become infected from having unprotected sex once or a person could have unprotected sex many times and not become infected, regardless of how low or high the risk per exposure is.
A risk of 1% would mean that an average of one infection would occur if 100 HIV-negative people were exposed to HIV through a certain type of sex. It does not mean that a person needs to be exposed 100 times for HIV infection to occur.
These are estimates of average risk in the absence of biological factors that increase risk.
The numbers in the table above are rough estimates. They are averages and do not represent the risk from all exposures to HIV through a certain type of sex.
We know that no two exposures to HIV are exactly the same. Research shows that, in addition to the type of sex that led to the exposure, several factors can increase or decrease the risk that an exposure to HIV leads to infection. These include the presence of sexually transmitted infections (STIs), a high viral load, a man being uncircumcised, a woman menstruating, other bleeding and activities that can cause tearing and inflammation, such as rough sex, longer sex, douching, enemas before anal sex, and tooth brushing, flossing or dental work before oral sex. Each exposure to HIV carries a unique risk of transmission that depends on the type of sex and a combination of biological factors.
The risk of HIV transmission may be much higher than these averages if biological risk factors are present. For example, research shows that STIs and some vaginal conditions, such as bacterial vaginosis, can increase the risk of HIV transmission by up to 8 times.6,7,8 As a result, the risk of an HIV-negative woman becoming infected through unprotected receptive vaginal sex could be closer to 1% (1 transmission per 100 exposures) if she has a vaginal STI.
We also know that for every 10-fold increase in viral load, the risk of HIV transmission increases by 2 to 3 times.9,10 Research suggests the extremely high viral load during acute HIV infection (the first few weeks after becoming infected with HIV) can increase the risk of HIV transmission by up to 26-fold.11,12 Therefore, unprotected sex with an HIV-positive person who has acute HIV infection could carry a transmission risk of up to 2% (the equivalent of 1 transmission per 50 exposures) for receptive vaginal sex and over 20% (equivalent to 1 transmission per 5 exposures) for receptive anal sex.
The more exposures, the greater the risk.
Although the risk of HIV transmission from a single exposure may seem low to some people, this risk increases over multiple exposures. In other words, a person who is exposed to HIV more often has a greater overall risk of HIV transmission than someone who is exposed less often.
If a woman has unprotected vaginal sex 100 times with a man who is HIV-positive, the cumulative risk is approximately 10% and may be higher if biological risk factors are present.
Differences in risk
Information on how risky certain types of unprotected sex are compared to others may help people make more informed decisions about the type of sex they are having.
- Receptive anal sex carries a much higher risk of HIV infection than receptive vaginal sex. Research shows that the risk of HIV transmission from receptive anal sex is up to 18 times higher than from receptive vaginal sex.
- Receptive anal sex is riskier than insertive anal sex. Research suggests the risk of HIV transmission from receptive anal sex is 3 to 23 times higher than from insertive anal sex.
- Receptive vaginal sex is riskier than insertive vaginal sex. The risk from receptive vaginal sex is about twice as high as that from insertive vaginal sex.
- It is unclear exactly how much less risky oral sex is compared to vaginal and anal sex.
Conclusion
Although it's impossible to provide a client with their exact risk of HIV transmission from an exposure, some studies have managed to estimate an average risk for different types of sex. It's important to provide clients with additional information to help them interpret the findings. Here are some key messages:
- These numbers:
- are challenging to calculate and should therefore be considered rough estimates
- do not represent the risk of transmission from all exposures to HIV
- represent the average risk of transmission in the absence of biological factors that can increase risk (such as STIs and a high viral load)
- are most relevant to people in stable monogamous serodiscordant relationships
- These numbers may seem low, but:
- HIV transmission can occur after a single exposure
- the risk may be much higher if certain biological risk factors, such as STIs or a high viral load, are present
- as more exposures to HIV occur, the overall risk of transmission increases
- most HIV transmissions in Canada occur through unprotected anal and vaginal sex
- There are several ways of reducing the risk of HIV transmission from an exposure, such as post-exposure prophylaxis (PEP), using antiretroviral treatment to reduce viral load, circumcision, treatment for STIs and vaginal conditions, or engaging in lower-risk activities.
- There is no way to reduce the risk of HIV transmission to zero after an exposure occurs. Taking measures to avoid an exposure in the first place (for example, through the correct use of condoms or other barrier methods, or by ensuring a partner has the same HIV status) can help reduce the overall risk of HIV transmission.
Footnotes - References
1. Baggaley RF, White RG, Boily M-C. HIV transmission risk through anal intercourse: systematic review, meta-analysis and implications for HIV prevention. International Journal of Epidemiology. 2010 Aug;39(4):1048–63.
2. Vittinghoff E, Douglas J, Judson F et al. Per-contact risk of human immunodeficiency virus transmission between male sexual partners. American Journal of Epidemiology. 1999 Aug 1;150(3):306–11.
3. Jin F, Jansson J, Law M et al. Per-contact probability of HIV transmission in homosexual men in Sydney in the era of HAART. AIDS. 2010 Mar 27;24(6):907–13.
4. a. b. Boily M-C, Baggaley RF, Wang L et al. Heterosexual risk of HIV-1 infection per sexual act: systematic review and meta-analysis of observational studies. Lancet Infectious Diseases. 2009 Feb;9(2):118–29.
5. Baggaley RF, White RG, Boily M-C. Systematic review of orogenital HIV-1 transmission probabilities. International Journal of Epidemiology. 2008 Dec;37(6):1255–65.
6. Ward H, Rönn M. Contribution of sexually transmitted infections to the sexual transmission of HIV. Current Opinion in HIV and AIDS. 2010 Jul;5(4):305–10. 7. Atashili J, Poole C, Ndumbe PM et al. Bacterial vaginosis and HIV acquisition: a meta-analysis of published studies. AIDS. 2008 Jul 31;22(12):1493–501. 8. Cohen CR, Lingappa JR, Baeten JM et al. Bacterial vaginosis associated with increased risk of female-to-male HIV-1 transmission: a prospective cohort analysis among African couples. PLoS Medicine. 2012 Jun;9(6):e1001251.
9. Wawer MJ, Gray RH, Sewankambo NK et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. Journal of Infectious Diseases. 2005 May 1;191(9):1403–9.
10. Baeten JM, Kahle E, Lingappa JR et al. Genital HIV-1 RNA predicts risk of heterosexual HIV-1 transmission. Science Translational Medicine. 2011 Apr 6;3(77):77ra29.
11. Wawer MJ, Gray RH, Sewankambo NK et al. Rates of HIV-1 transmission per coital act, by stage of HIV-1 infection, in Rakai, Uganda. Journal of Infectious Diseases. 2005 May 1;191(9):1403–9. 12. Hollingsworth TD, Anderson RM, Fraser C. HIV-1 transmission, by stage of infection. Journal of Infectious Diseases. 2008 Sep 1;198(5):687–93.
About the author(s)
James Wilton is the Project Coordinator of the Biomedical Science of HIV Prevention Project at CATIE. James has an undergraduate degree in Microbiology and Immunology from the University of British Columbia.
Condition Spotlight
Clinical Trials
Clinical trials are research studies that evaluate a new medical approach, device, drug, or other treatment. As a Stanford Health Care patient, you may have access to the latest, advanced clinical trials.
Open trials refer to studies currently accepting participants. Closed trials are not currently enrolling, but may open in the future.